Muhammad Shoaib Khan1,
Ajwad Khan1,
Atif Ali2 ![]() ,
Naveed Akhtar1,
Fatima Rasool3,
Hira Khan1,
Nisar ur Rehman2,
Sajid Hussain Shah4
,
Naveed Akhtar1,
Fatima Rasool3,
Hira Khan1,
Nisar ur Rehman2,
Sajid Hussain Shah4
For correspondence:- Atif Ali Email: ajmaline2000@gmail.com
Received: 7 February 2015 Accepted: 29 August 2015 Published: 29 January 2016
Citation: Khan MS, Khan A, Ali A, Akhtar N, Rasool F, Khan H, et al. Prevalence of risk factors for coronary artery disease in Southern Punjab, Pakistan. Trop J Pharm Res 2016; 15(1):195-200 doi: 10.4314/tjpr.v15i1.27
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose:To explore the prevalence of risk factors for coronary artery disease (CAD) in Southern Punjab, Pakistan.
Methods:A cross-sectional survey was conducted for the prevalence of risk factors for CAD among 200 patients admitted at the different hospitals of Southern Punjab, Pakistan from December 2012 to April 2013. A questionnaire was used to collect data, including demographic information, family health history, dietary habits, physical activity and tobacco use. History of hypertension, diabetes mellitus (DM) or its treatment was recorded after observing their medical reports.
Results:The proportion of females and males was 65.53 and 34.46 %, respectively. Of the 200 patients, the mean age of males was 52.7 years and 55.8 years for females. The most prevalent coronary artery risk factors were physical inactivity (52.5 %), hypertension (52 %), poor dietary habits (48.5 %), fatty food consumption (47.5 %), obesity (38 %) and smoking (37 %), respectively. Other less common risk factors were diabetes (30 %) and family history of CAD (20 %).
Conclusion:CAD was seen in only 20 % of the subjects; the prevalence of individual risk factors ranged from 30 to 52.5 % and can be improved by encouraging the patients to adopt a healthy life style.
Introduction
Progressive expansion and acceptance of a western life style contributes to the rising burden of cardiovascular disease (CVD) in the developing world, including Pakistan [1]. The ‘exclusive’ disease, which was once restricted to the wealthy class, is now increasingly involving people from lower socio-economic sections especially the younger age groups [2]. The risk factors of CAD, if identified at an early stage can be extremely useful in planning primary and secondary preventive strategies. A major chunk of government resources can be saved which would otherwise be spent for investigation and treatment of patients with CAD and its complications [3].
In South Asia the prevalence of hypertension is 3.2 %, diabetes 2.6 %, and CAD is 3.2 %. However, in urban and immigrant populations the prevalence rates are 12 – 20, 6 – 8, and 7 – 14 %, respectively. Mean serum cholesterol level is 180 – 200 mg/dL, frequency of obesity 5 – 8 % and dietary fat intake contains 20 – 30 % of total calorie intake [4]. Several subgroups of South Asia do have high smoking rates, especially in urban areas. Among the known risk factors, levels of HDL-c have been found to be inherently low in the normal South Asians population. Low HDL-c alone or in combination with high levels of LDL-c, insulin resistance and hypertension constitute a very important intermediate phenotype for CAD. In a recent study on young myocardial infarction patients, 70.3 % were found to have HDL-c lower than 40 mg/dL [5].
Despite the fact that it is the developing world that will most likely face the epidemic of hypertension (HT) and other chronic diseases [6], Research on cardiovascular diseases in a developing country such as Pakistan has been limited.
This study used a population based survey to measure the prevalence of different CAD risk factors in a Southern Punjab population sample where little is known about CAD, the disease load, and risk factors.
Methods
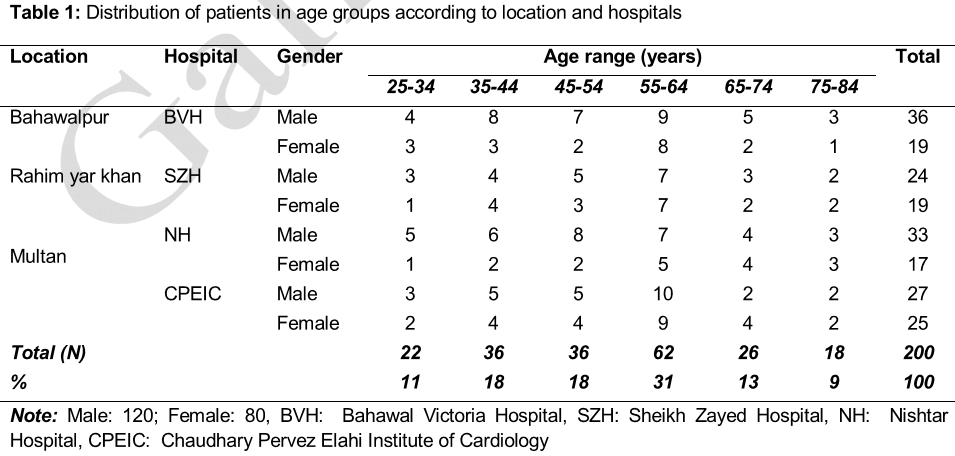
This study was conducted at the Bahawal Victoria Hospital, Bahawalpur, Sheikh Zaid Hospital, Rahim Yar Khan, Chaudhary Pervez Elahi, Institute of Cardiology and Nishtar Hospital, Multan. In addition, these hospitals are large government hospitals of major cities of Southern Punjab- Pakistan. The study (Reference No. 366) was approved from the Ethical Institution Committee, Department of Pharmacy and the Islamia University of Bahawalpur, Bahawalpur- Pakistan.
Population study
This study was conducted from December 2011 to April 2012 and comprised 200 patients. The patients included in the survey were suffering from acute myocardial infarction and/or they were diagnosed with CAD. They were divided into 6 age groups: 25 - 34, 35 - 44, 45 - 54, 55 - 64, 65 - 74 and 75 - 84 years old. All eligible participants gave informed agreement.
Data collection
The authors prepared questionnaires used to collect such data as demographic information, family health history, dietary habits, physical activity and tobacco use. History of hypertension or its treatment, histories of diabetes mellitus (DM) or its treatment were recorded after observing their medical reports.
Demographic information comprised sex and age of subjects. Family health history included the presence of CAD in immediate family of patients (mother, father, brother, sister). Dietary history included a subjective account of daily fat and fruit intake. Timing and frequency of meal intake was also recorded. Physical activity was assessed by the occupation and daily physical workout which includes walk for 30 min or the medium of frequent travelling (bicycle, bike or car). Tobacco use was assessed by asking the patient if he was an active smoker, passive smoker, non-smoker or quitter. If the patient was an active smoker or quitter then he was asked then for how long he had been smoking and how many cigarettes he/she smoked per day.
History of DM and hypertension were positive if a participant has ever been told by a physician to have DM or hypertension or treated accordingly and the medical reports were also checked for further evidence of DM and hypertension if they were available.
Anthropometric features were also recorded which included weight, height, and body mass index (BMI). The weight of participants was determined in subject without foot wear and light clothing using a portable Weighing scale and the height accurately measured with inches tape. Then the BMI was calculated using formula:
Traditional risk factors were defined as follows:
Obesity: BMI > 30
Overweight: BMI, between 25 – 29.9
Hypertension: Currently taking antihypertensive medications and/ or systolic blood pressure (SBP) > 140 and/or diastolic blood pressure (DBP) > 90, by taking the mean of 4 measurements.
Diabetes mellitus: history of using hypoglycemic agents and/or fasting blood sugar (FBS) > 126 and glucose tolerance test (GTT) > 200.
Smoking: consumption of 10 cigarettes per day at least for 3 months.
A person is considered to have an inactive behavior if he walks less than 4-5 km a week, climbs fewer than 20 flights of stairs a week or performs no moderate physical activity (300 Kcal/day) on 5 days a week.
CAD was diagnosed if the patient had coronary angio-graphic evidence of significant CAD with a greater than 50 % obstruction of at least one major coronary artery, a documented myocardial infarction or typical angina pectoris.
Statistical analysis
Chi square test was applied to analyze the data by Statistical Package for Social Sciences 17.0 software (SPSS). The level of significance was 5 %.
Results
Prevalence of modifiable and non-modifiable risk factors for CAD, i.e. fatty food consumption, less fruit intake, smoking, obesity, exercise, hypertension, diabetes and family history of CAD was assessed among patients diagnosed with coronary artery disease at a hospital. There is a scarcity of reliable community based epidemiological data on the prevalence of CAD from Southern Punjab and even less is known regarding the prevalence of CAD in the community setting. The 200 participants aged from 25 to 84 years with mean age of 52.7 years in male and 55.8 in female as shown in .
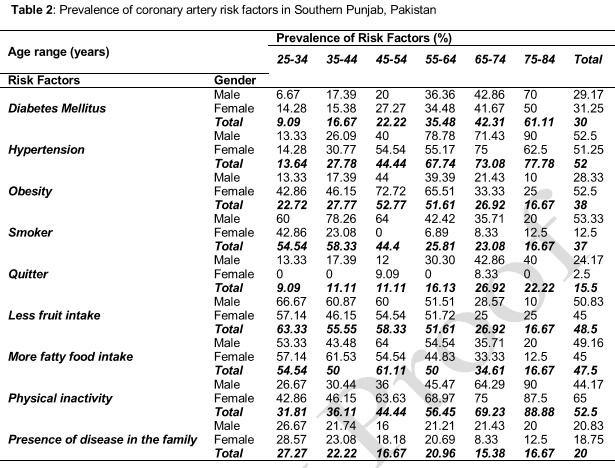
Family history of CAD was found in 20 % of the total subjects. Presence of family history of CAD in the families of male subjects was 20.83 % and in females was 18.75 %. The present study revealed that the most prevalent coronary artery risk factors in Southern Punjab were physical inactivity (52.5 %), hypertension (52 %), poor dietary habits (less fruit intake (48.5%) and more fatty food consumption (47.5 %), obesity (38 %) and smoking (37 %), respectively. Other less common risk factors were diabetes (30 %) and family history of CAD (20 %). Almost all of the subjects had more than one CAD risk factors. Based on 10-year age intervals of 25 - 34, 35 - 44, 45 - 54, 55 - 64, 65 - 74 and 75 - 84, the prevalence of CAD risk factors were standardized based on age and sex distribution of Southern Punjab population. Prevalence of risk factors for CAD in Southern Punjab was given in .
Physical inactivity was higher in females (65 %) as compared to males (44.17 %). As age increased physical inactivity decreased i.e. 31.8 % in 25 - 34 year age group while 69.23 % in 65 - 74 year age group and 88.88 % in 75 - 84 year age group. According to the outcomes, the total prevalence of hypertension was 52 % (52.5 % in men and 51.25 % in women). Again the prevalence of hypertension increased with age in both genders. Physical inactivity was prevalent among females by 65 % as compared to 44.17 % in male population.
Less fruit consumption was seen in subjects in lower age groups. As age increased, there was less fruit intake (26.92 % in 65-74 year and 16.67 % in 75 - 84 year age groups).
47.5 % of the total patients had more fatty food intake rich in cholesterol. The trend of fat intake was slightly higher in males (49.16 %) as compared to females (45 %). Subjects in lower age group i.e. 25 - 34, 35 - 44, 45 - 54 years tended to have higher fat intake. Fatty food consumption decreased as the age increased. It was lowest in 75 - 84 year age group (16.67 %).
Discussion
The rise in CVDs reflects a significant change in diet habits, physical activity levels, and tobacco consumption worldwide as a result of industrialization, urbanization, economic development and food market globalization [1]. The American Heart Association has recently focused on physical inactivity as a major modifiable risk factor for heart disease [7]. Prevalence of physical inactivity among females was more because most of the women were housewives with low physical activity. As the age increased physical activity declined. This finding highlights a potential area of emphasis for future educational programs [8].
One study [9] has shown that consumption of fruits and vegetables, particularly green leafy vegetables and vitamin C–rich fruits and vegetables, appear to have a protective effect against coronary heart disease. Many mechanisms are likely responsible for the protective effect of plant-origin foods on cardiovascular diseases. Several epidemiologic studies have reported that vitamins C, E, and β-carotene from the diet or supplements are associated with a lower risk of CHD [10,11].
Saturated fat intake has been related to acute myocardial infarction in adults [12]. Subjects who use ghee for cooking compared with other types of non-hydrogenated oils, a higher percentage of Trans fatty acids, known to increase the risk of ischemic heart disease [13-15], has been reported.
In Pakistan, where there is also a problem of under nutrition, in 1994 11.6 % males and 18.93 % females were obese or overweight (WHO global database on BMI). The prevalence of obesity, i.e. having BMI greater than 30 was 38 % in Southern Punjab. Overall, 28.33 % of men and 52.5 % of women had excess weight. The prevalence of obesity, which is strongly associated with CAD, was higher in females. The prevalence of obesity was significantly higher in the subjects of age group 45 - 54 year old (52.77 %) and 55 - 64 year old (51.61 %) as compared to other age groups. Low physical activity and eating habits may be relevant factors that explain the difference between males and females [7].
Almost one-half billion individuals worldwide will eventually die of smoking-related complications [16]. 37 % of subjects were cigarette smokers. The prevalence of smoking was significantly higher in men (53.33 %) as compared to women (12.5 %). The highest prevalence of smoking was in the 35 - 44 year old men (78.26 %). Compared with non-smokers, those who consume 20 or more cigarettes daily have a twofold to threefold increase in total coronary heart disease. Moreover, these effects depend on the number of cigarettes consumed; consumption of as few as one to four cigarettes daily increases coronary artery disease risk, while 15.5 % of the subjects were those who had quit smoking. Number of quitters increased with increasing age, with the highest of 26.92 % in 65 - 74 year age group. Again most of the quitters were men (24.17 %) as compared to women (2.5 %). Number of smoking quitters increased with increasing age with the highest in men of 65 - 74 year age group (42.86 %).
Pakistan is one of the 10 countries in the world with the highest prevalence of diabetes and has one of the fastest increases in the number of diabetics [17]. The present investigation revealed that about one-third of the 25 - 84 years old population of Southern Punjab is diabetic, 29.17 % in men and 31.25 % in women. Aging had an increasing influence on the prevalence of diabetes. DM increased from 9.09 % in the 25-34 year old group to 61.11 % in the 75 - 84 year old subjects. More females were diabetics, although not significantly different as compared to males. This high prevalence in females may be due to low physical activity and/or increase trend in obesity. However, environmental factors such as dietary patterns are more likely to be shared among family members, and this effect will probably be stronger in consanguineous relationships [18].
Limitation of the study
The study was cross-sectional and therefore, the directionality of the associations could not be determined.
Conclusion
Various risk factors for CAD are highly prevalent in the study population. Though the history of CAD was available in only 20 % of the subjects, the prevalence of individual risk factors ranges from 52.5 to 30 % and approximately all of the subjects have more than one risk factor. Most of these risk factors are modifiable and can be improved by encouraging the patients to adopt a healthy life style such as reducing daily fat intake, increasing fruit and vegetable intake, quitting smoking and engaging in more physical activities. Besides this, screening the community for the presence of diabetes and hypertension combined with proper intervention can reduce morbidity and mortality from this disease.
Declarations
Acknowledgement
References
Archives


News Updates