Maxwell O Adibe ![]() ,
Nneka U Igboeli,
Chinwe V Ukwe
,
Nneka U Igboeli,
Chinwe V Ukwe
For correspondence:- Maxwell Adibe Email: Maxwell.adibe@unn.edu.ng Tel:+2348037781479
Received: 13 June 2016 Accepted: 8 July 2016 Published: 31 March 2017
Citation: Adibe MO, Igboeli NU, Ukwe CV. Evaluation of drug therapy problems among renal patients receiving care in some tertiary hospitals in Nigeria. Trop J Pharm Res 2017; 16(3):697-704 doi: 10.4314/tjpr.v16i3.27
© 2017 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To determine the prevalence of drug therapy problems (DTPs), identify the types of DTPs and assess outcomes of DTP interventions among renal patients receiving care in three Nigerian tertiary hospitals.
Methods: This prospective descriptive study was conducted in nephrology units of three tertiary hospitals in Nigeria, based on recommendations of working conference of the Pharmaceutical Care Network Europe, version 6.2 while the reviews, classification of DTPs and principles of drug use in chronic kidney diseases (CKD) were based on evidence-based clinical guidelines and standards of practice (Kidney Disease: Improving Global Outcomes (KDIGO).
Results: Out of 234 DTPs identified, 90 (38.46%) had drug choice problem, 86 (36.75%), had problems of drug interactions; 47(20.09%), had dosing problem, while 11 (4.70%) had drug use problem. Clinical interventions (459) were undertaken at prescriber level (78; 16.99%); patient/carer level (211, 46.00 %) and drug level (170, 30.04 %). Pharmacists recommended 376 of the interventions for approval, out of which 310 (67.54%) were approved. Amongst the DTPs indentified, 47.86 % were successfully resolved.
Conclusion: Drug therapy problems among renal patients were high. Inappropriate drug selection and drug interactions were the commonest drug therapy problems. The acceptance of pharmacists’ interventions by prescribers was appreciable
Introduction
Medications intended for the treatment, prophylaxis or diagnosis of medical conditions may have negative effects on patients if not used appropriately. Over the years, there have been numerous reports of incidence, prevalence, and preventability of drug-related hospital admissions [1-3], medication error-related deaths [4], and adverse drug events in in-patient and out-patient settings [5-7]. Drug‑related problems are common in hospitalized patients and can interfere with the achievements of desired therapeutic outcomes [8]. These problems can potentially have an impact on desired health outcomes [9]. Due to their training, pharmacists can play an important role in identifying these drug therapy problems (DTPs), resolving actual DTPs and preventing potential DTPs through careful pharmaceutical practices. There is increasing evidence that participation and interventions of clinical pharmacists in health care have a positive influence on clinical practice [10]. In a number of studies, clinical pharmacists have been shown to reduce DRPs in the in-patient settings [11]. Some publications have evaluated the impact of drug errors identified or intercepted by pharmacists in emergency departments [12-14], and in in-patient medical and surgical wards [15,16].
In CKD, the number and complexity of drugs increase with the progression of the disease and can result in a high risk of non-compliance and adverse drug reactions. Moreover, CKD patients are more at risk of iatrogenic renal failure than non-CKD patients (15.3 % vs. 5.3 %, respectively) when admitted to an intensive care unit [17]. Several studies have shown that patients with end-stage renal disease (ESRD) are among those at high risk for DTPs [18,19].
The objectives of this study were to determine the prevalence of DTPs, identify the types of DTPs, and assess the outcomes of DTP interventions among renal patients receiving care in three Nigerian tertiary hospitals.
Methods
Study design and setting
This prospective descriptive study was conducted in nephrology unit of University of Nigeria Teaching Hospital (UNTH), Enugu; Nnamdi Azikiwe Teaching Hospital, Nnewi and Enugu State University Teaching Hospital. These are tertiary hospitals that serve as referral centres to most of the hospitals, in particular, in South-Eastern geo-political zone of Nigeria. Ethical clearance of the study was obtained from each hospital ethics committee prior to data collection.
Study participants
The study included all renal patients who were diagnosed with acute renal failure, chronic renal failure and other kidney related diseases; 18 years and above, with or without co‑morbidities, and on admission to the medical ward for kidney-related problems from October, 2014 to March, 2015.
Instruments for study
This study protocol was based on the recommendation made during the working conference of the Pharmaceutical Care Network Europe, a classification scheme constructed for drug related problems (DRPs, V6.2) [20].
The questionnaire used in this study had information on the patient’s demographic characteristics, including age, sex, and medical history, drugs administered to the patient during the hospitalization period: Drug name, indication, dose, schedule, duration, and monitoring, stage of CKD, associated co-morbidities, length of hospital stay, and number of drugs prescribed, and the type of DRPs and pharmacist’s interventions.
Data collection
Identification and classification of potential and actual DRPs using appropriate guidelines was assessed by 3 clinical pharmacists through review and analyses of all medication orders, administration sheets, laboratory and diagnostic test results and pathophysiological status. Patients were interviewed for relevant information for the study. The reviews, classification of DTPs and principles of drug use in the CKD were based on evidence-based clinical guidelines and standards of practice [21,22]. These guidelines have sections for use of drug in patients with CKD in reference to other co-morbidities, CKD progression/staging and dosage adjustment charts and DTPs in CKD for individual drugs or groups of drugs.
Drug-drug interactions were assessed using RxList drug interaction platform [23]. The RxList identifies how the number of interactions in a prescription and rates them into the following categories:
Each patient’s drug therapy was routinely monitored in every follow-up appointment and the DRPs were identified, discussed, and documented by the panel. The DTPs and other medical related matters were unanimously agreed upon during a round table discussion by panel members (differences were resolved by consensus). Intervention involved discussion of resolution of the problem with the prescribers, counselling and educating the patients as appropriate and change or discontinuation of the drug. Drug therapeutic problem charts were collected, analyzed, and categorized into types of problems, causes of problems, interventions, and outcomes of interventions. The medication therapy review was tailored to the individual problems of the patient at each encounter. Following identification of any DTPs, an intervention was proposed to the patient, or the physician or other healthcare professionals, or both, as appropriate so as to optimize therapy. The communication of appropriate information to the physician or other healthcare professional including consultation on the selection of medications, correct dosage regimens, suggestions to address medication problems, recommendations and outcomes were documented.
Data analysis
The data were collated and entered into version 21 of SPSS (SPSS Inc. Chicago) and Microsoft 2007 Excel package for analysis. Descriptive statistics was done and continuous variables were expressed as means ± standard deviation.
Results
Patients socio-demographic characteristics
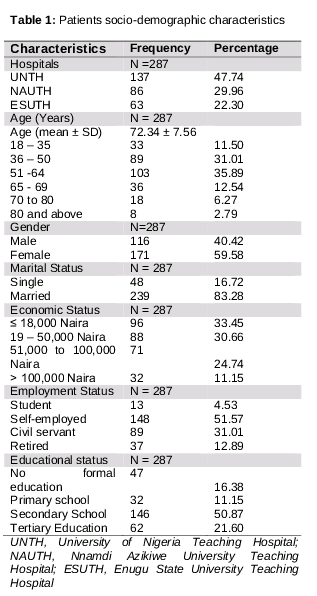
A total of 287 patients with renal illnesses were followed for five months and assessed for DTPs. More than half of the patients were above 50 years old (165, 57.49 %), out of which 171 (59.58 %) were female. Majority of patients were married (239, 83.28 %) and about one third of them earned less than ₦18, 000 monthly ().
Patients’ clinical variables
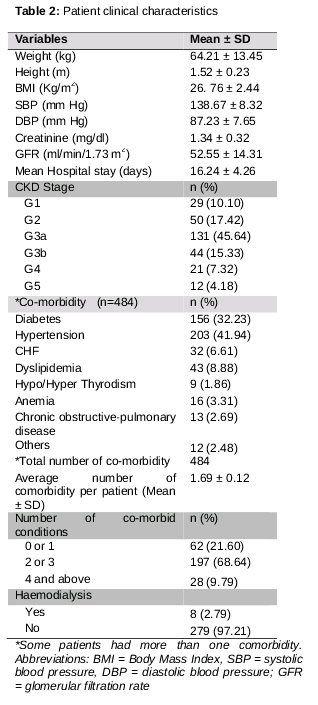
The clinical features of the patients showed that mean serum creatinine, Glomerular Fitration Rate (GFR) and hospital stay were 1.34 ± 0.32 mg/dl, 52.55 ± 14.31 ml/min/1.73 m2 and 16.24 ± 4.26 days, respectively. The number of patients with CKD stages G3 to 5, was 208 (72.48 %). A total of 484 co-morbidities (mean: 1.69 ± 0.12) were documented, with hypertension and diabetes accounting for about two-thirds of the co-morbid conditions. Most of the patients (197, 68.64 %) had 2 or 3 co-morbid conditions ().
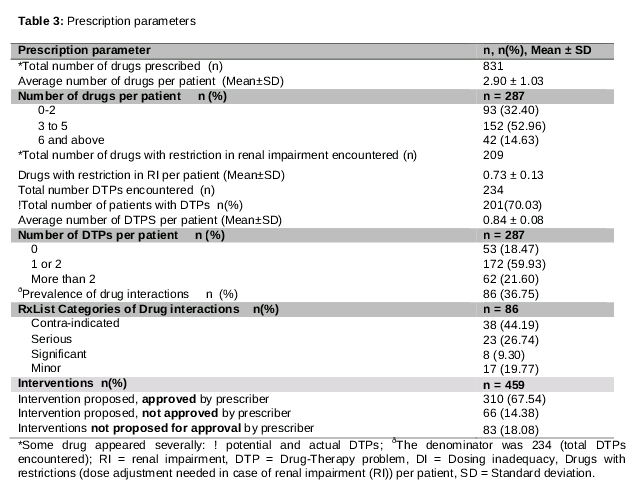
The total number of drugs received by patients was 831 and the number of drugs in the prescriptions of most patients (52.96%) ranged from 3 to 5 with an average of 2.90 ± 1.03 per patient. The number of drugs with restriction in renal impairment (RI) was 209, with an average of 0.73 ± 0.13 drugs per patient ().
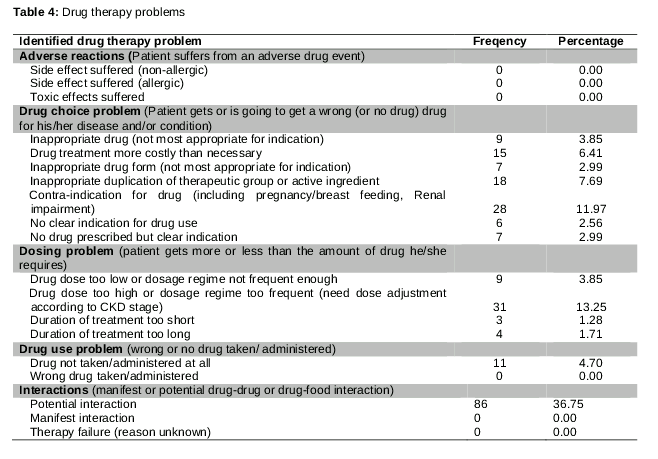
Amongst the 201 patients with DTPs, 234 DTPs were identified in following descending order of their prevalence ‘drug choice problem’: 90 (38.46 %); ‘drug interactions’: 86 (36.75 %); ‘dosing problem’ 47 (20.09 %); drug use problem: 11 (4.70%) and adverse drug reaction: 0 (0.00%). The detailed results showed that top specific causes of DTPs were ‘potential drug interactions (36.75 %) and ‘drug dose too high or dosage regime too frequent’ ().
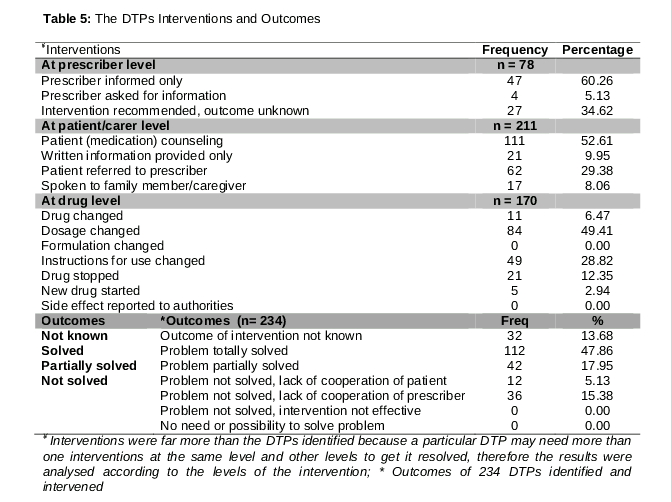
A total of 459 clinical interventions were undertaken at three levels of the intervention: prescriber level: 78 (16.99 %); patient/career level: 211 (46.00 %) and drug level: 170 (30.04%). Out these, ‘prescriber informed only’ (47, 60.26 %), ‘patient (medication) counselling’ (111, 52.61 %) and ‘dosage changed’ (84, 49.41 %) were the most recommended for intervention at each level. Out of the 459 interventions, 376 (81.91 %) were recommended for approval from the prescribers, out of which 310 (67.54 %) were approved ().
Of the 234 DTPs identified, ‘problems totally solved’ was 112 (47.86 %), ‘partially solved’ was 42 (17.95%), ‘problem not solved due to lack of cooperation of the patient’ was 12 (5.13%), ‘problem not solved due to lack of cooperation of prescriber’ was 36 (15.38%) and ‘outcomes not known’ was 32 (13.68 %), .
Discussion
This study has revealed a very high proportion (70.03%) of CKD patients with DRPs. Out of the 67.54 % of interventions by pharmacist approved by a panel, 47.86 % of the DTPs identified were successfully resolved. This high proportion of DTPs might be due to relatively older population involved in the study, as well as severe CKD and multiple co-morbidities among the renal patients.
Increasing age causes increasing vulnerability to diseases and, in the elderly, the tendency to acquire multiple and chronic diseases. This population therefore is prescribed and uses more drugs than younger populations. In addition, multiple complaints, atypical disease presentation and physician prescribing habits and practices have resulted in the use of multiple drugs by these patients [24]. Age is one of the most important underlying risk factors for CKD, often compounded by the presence of other co-morbidities such as diabetes, hypertension and vascular disease. Among healthy individuals, creatinine clearance peaks at approximately 120-130 mL/min/1.73m2 at age 30 years and then declines by about 8 mL/min/1.73m2 per decade [21].This result is in agreement with the findings in an earlier study [25], which showed that majority of patients with DTP were 60 years and above.
Most of the patients in this study had CKD stage 3-5 which requires a therapeutic intensification to slow the progression of the disease, prevent risk of acute kidney injury and treat co-morbidities, particularly cardiovascular risk factors [26]. In doing these, there is need to pay close attention on the GFR of the patients, to make sure the CKD stage does not go beyond G2: this study had shown a significant likelihood of increase in the number of DTPs by 6.52 for every additional deteriorating stage, provided the patients are of the same in other variables.
More than one-quarter of the patients had at least 4 co-morbidities and about two-thirds received at least 3 medications. While no specific number of medications has been established to define polypharmacy, some have arbitrarily suggested cut-off points of 3 to 5 drugs per patient [27]. Our results appear to conform with this, since 14.63% of the patients received 6 or more drugs. In addition, the patients included in this investigation had several risk factors for polypharmacy, including older age, renal disorders, and poorer health [27].
This revelation underscores the need for extra vigilance while reviewing patient’s drugs as this could increase their DTPs and cost. A total of 234 drug therapy problems (DTPs) were identified which resulted from drugs prescribed during the study. This is considered high. Although Ramalho de Oliveira et al [28] identified 38,631 DTPs over a period of 10 years, 380 DTPs were identified by Nascimento et al [29] in a period of two years, and Root et al [30] identified 88 DTPs from 40 patients. The difference in the number of DTPs encountered is probably due to differences in research design in terms of patients type, hospital types, duration of the studies and nature of data collected.Our study showed that mean drug per patient was almost 3.0 which is moderate, despite the involvement of older population of patients in this study. This might be due the fact that most of the DTPs encountered in the hospital were not recorded or were even missed by pharmacists.
Inappropriate drug selection/dosing problem and drug interaction were the major sources of DTPs in this study. This result is consistent with a number of studies [25,29-33] on DTPs in which dosing and/or drug selection problems and drug interaction were identified among the major forms of DTPs encountered.
A high number of DTPs due to drug choice/selection and potential drug interactions was recorded in our study. This is similar to results obtained in a study conducted by Ismail et al [34] which showed 45 % potential drug‑drug interactions at pulmonology ward in a tertiary care hospital at Peshawar, Pakistan. Our results confirm that drug‑drug interaction is a common drug therapy problem in both government and private hospitals. Khan et al [35] and Alagiriswami et al [36] also reported high incidence of drug selection problems.
The result of this study also revealed that the number of interventions was highest at patient/career level, followed by drug level and least at prescriber level. This is in agreement with the data from a 10-year study by Ramalho et al [28] where 80% of DTPs identified in Fairview’s MTM programme were resolved at the drug or patient level without the direct involvement of physician(s).
The trend of recommendation approval found in this study is also similar to the results of Root et al [30] where 75 % of the pharmacists’ proposed interventions were approved. The lower rate of approval of proposed intervention obtained in the current study could be as a result of lack of collaboration between healthcare providers.
Appreciable number of DTPs identified were totally resolved. Just like in many studies where pharmaceutical care interventions were instituded [28-30], DTPs were resolved, patients’ conditions were improved and consequently the rate of encoutered DTPs in that setting was reduced. This is predicated in high acceptance of the intervention by the doctors. Pharmacists in this hospital should embrace this opportunity to reach out to patients who are greatly in need of their attention; no matter how busy they are, especially in this era of ever expanding role of a pharmacist.
The present study has several limitations and the results are interpreted in this light. The approach used to identify and classify DTPs was based on record reviews and explicit criteria of the applied guidelines. We could not account for information other than those in patients’ records and those reported to us. Likewise, we focused on regularly scheduled medications rather than on as-needed drugs. Thus, our findings may be biased toward reporting more of the easily identifiable DTPs.
Conclusion
Drug therapy problems among the renal patients studied were high. Inappropriate drug selection and drug interactions were the commonest drug therapy problems. Pharmacists in Nigerian hospitals should always reach out to all patients to identify and resolve any drug-related problems associated with the patients’ medications.
References
Archives


News Updates